
ZFTA–RELA ependymomas make itaconate to epigenetically drive fusion expression
Article meta
Article Date: 04 February 2026
Article URL: https://www.nature.com/articles/s41586-025-10005-1
Article Image: Figure 1
{kind=link}
Summary
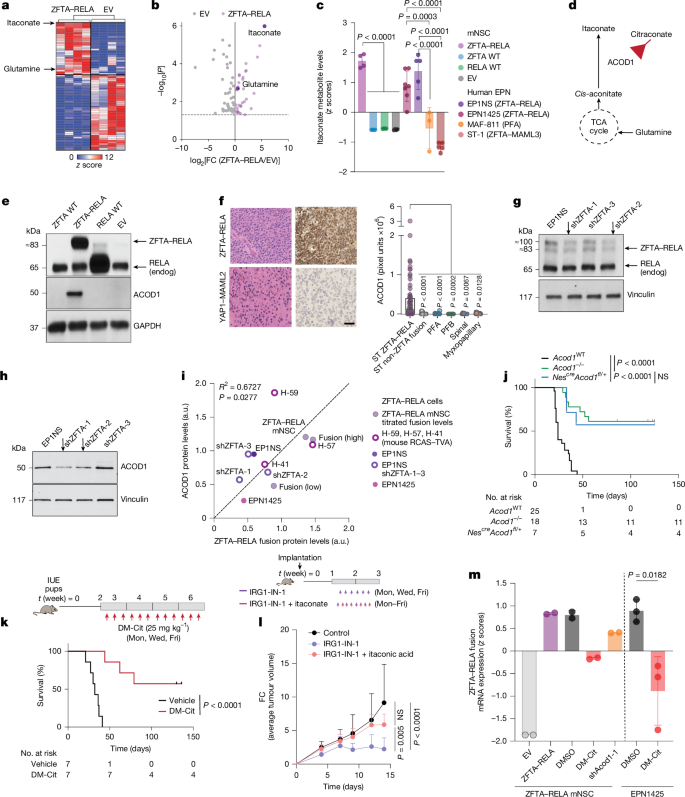
This Nature study shows that ZFTA–RELA fusion-positive supratentorial ependymomas reprogramme metabolism to produce the macrophage metabolite itaconate. The fusion upregulates ACOD1 (IRG1), driving itaconate synthesis from glutamine-fed TCA cycle intermediates. Itaconate acts as an epigenetic modifier — inhibiting αKG-dependent demethylases (notably KDM5) to boost H3K4me3 at regulatory sites that sustain ZFTA–RELA transcription. Genetic or pharmacological blockade of ACOD1, or targeting glutamine metabolism (SLC1A5/GLS inhibitors, glutamine antagonists like JHU-083), reduces itaconate, lowers global H3K4me3, decreases ZFTA–RELA levels and suppresses tumour growth in multiple mouse and PDX models. The fusion also epigenetically represses PTEN to activate PI3K–AKT–MYC signalling, increasing GLS/SLC1A5 and creating a glutamine dependency that can be exploited therapeutically.
Key Points
- ZFTA–RELA+ ependymoma cells upregulate ACOD1 and produce itaconate at levels comparable to activated macrophages.
- Glutamine is the main carbon source feeding itaconate synthesis in these tumours via the TCA cycle.
- Itaconate inhibits KDM5 histone demethylases, raising H3K4me3 and sustaining ZFTA–RELA fusion transcription through ZFTA regulatory elements.
- Genetic loss or pharmacological inhibition of ACOD1 (shRNA, IRG1-IN-1, dimethyl citraconate) lowers H3K4me3, reduces ZFTA–RELA mRNA/protein and suppresses tumour growth and metastasis in vivo.
- ZFTA–RELA epigenetically represses PTEN, activating PI3K–AKT–mTOR and MYC to boost GLS and SLC1A5, enforcing glutamine addiction.
- Targeting glutamine metabolism (V9302, CB-839, DON, CNS-penetrant JHU-083) or PI3K–mTOR (PI-103) — alone or combined — reduces tumour growth, lowers fusion protein levels and improves survival in models.
- Mutating KDM5 recognition sites at the ZFTA regulatory region increases fusion expression and confers resistance to itaconate antagonism, supporting an epigenetic mechanism.
Why should I read this?
Short version: these nasty brain tumours hijack metabolism to make itaconate, which in turn keeps the oncogenic fusion switched on. Block the pathway and the fusion falls apart. If you’re into new, druggable angles on aggressive ependymoma — or want a neat example of metabolism directly rewiring epigenetics — this paper is gold. It’s dense with models and translational experiments, so the details matter if you’re considering therapeutic strategies or follow-up studies.
Author style
Punchy: this is a big translational find. The authors combine metabolomics, isotope tracing, epigenomics and multiple in vivo models to map a coherent metabolic→epigenetic feed‑forward loop that sustains the pathogenic ZFTA–RELA fusion — and they show several ways to break it. Read the full text for experimental nuance and therapeutic caveats; the headline is promising but clinical translation will need safety and CNS delivery work.
Context and relevance
This work positions itaconate as a tumour-produced oncometabolite, analogous to 2‑HG or fumarate, linking metabolism to chromatin regulation in ependymoma. It reveals multiple actionable nodes — ACOD1, glutamine uptake and GLS, and PI3K–mTOR signalling — that are already targetable with existing inhibitors or prodrugs (notably a CNS-penetrant glutamine antagonist). That makes the study highly relevant to researchers and clinicians seeking new targeted strategies for ZFTA fusion ependymomas, a group that currently lacks effective targeted therapies.
Limitations and next steps (brief)
Preclinical only: results are robust across cell lines, PDXs and genetic models but human safety, blood–brain barrier pharmacology and tumour microenvironment/immune effects (itaconate is immunomodulatory) need careful study. Clinical-grade ACOD1 inhibitors and CNS-penetrant combinations will be the obvious next steps.