
Individualized mRNA vaccines evoke durable T cell immunity in adjuvant TNBC
Article Date: 18 February 2026
Article URL: https://www.nature.com/articles/s41586-025-10004-2
Article Image: Figure 1
{kind=link}
Summary
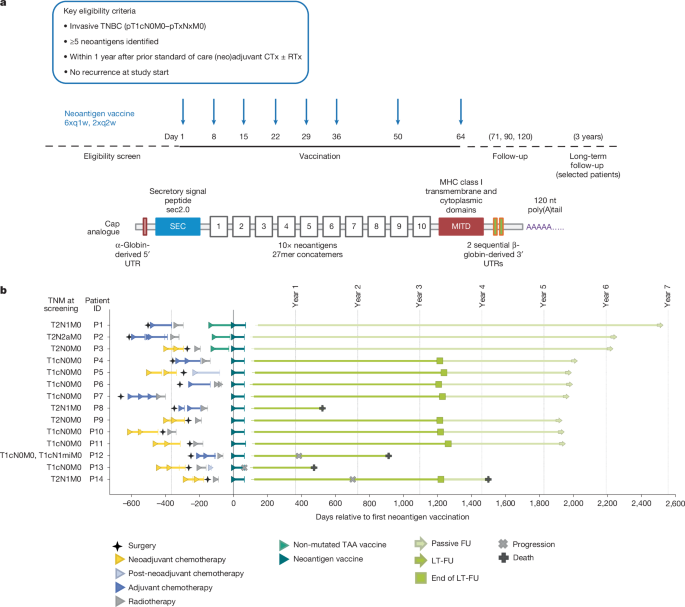
This first-in-human arm of the MERIT umbrella trial tested an individualized uridine mRNA–LPX neoantigen vaccine in patients with early triple-negative breast cancer (TNBC) after standard (neo)adjuvant therapy. Tumour sequencing guided on-demand GMP manufacture of two RNA molecules encoding up to 20 patient-specific neoantigens; vaccines were delivered intravenously in liposomal nanoparticles. Fourteen patients completed per-protocol vaccination (eight doses, final dose at day 64). The vaccine platform was feasible to produce (mean turnaround ≈69 days), was generally well tolerated (mainly transient, low-grade reactogenicity), and induced neoantigen-specific T cell responses in every evaluable patient.
Vaccine-induced responses were often poly-epitopic and high magnitude: most patients mounted T cell responses to multiple vaccine targets, with ex vivo IFNγ ELISpot positivity in ~86% of participants. Both CD8+ and CD4+ responses were observed; many CD8+ clones reached single-digit percentages of circulating CD8+ T cells. Responses expanded during vaccination, contracted slightly, then stabilised and—critically—many persisted long term (months to years). Detailed TCR and single-cell profiling (notably in patient P1) showed durable, functional cytotoxic and stem-like memory T cell populations detectable up to 6 years. At median follow-up of ~62 months, 10/14 patients remained relapse-free. Failures illustrated likely escape routes: poor initial immune induction, independent synchronous tumours (BRCA case), or immune evasion via loss/downregulation of antigen presentation (B2M/MHC-I loss).
Key Points
- Personalised uridine mRNA–LPX neoantigen vaccines (up to 20 targets) are clinically feasible to manufacture and deliver after standard TNBC treatment.
- Vaccination was well tolerated; adverse events were mainly transient, grade 1–2 reactogenic symptoms (fever, headache, chills, nausea, fatigue).
- All 14 evaluable patients mounted vaccine-induced or amplified T cell responses against at least one vaccine neoantigen; most patients responded to multiple targets.
- High-magnitude CD8+ responses were common (some neoantigen-specific clones reached >5–10% of circulating CD8+ cells), and many responses were polyfunctional.
- Neoantigen-specific T cells showed durable persistence (months to years), evolving into effector-memory and stem-like memory phenotypes with self-renewal markers (TCF1, IL7Rα).
- Long-term clinical status: 10/14 patients relapse-free at median 62 months follow-up; relapses highlighted immune escape mechanisms such as loss of MHC class I/B2M and independent tumour origins.
- On-demand GMP manufacturing workflow is feasible in a standard clinical setting (average turnaround ≈69 days), though not yet optimised for speed.
- Study limitations: small cohort size, no control arm, and limited PBMC/sample availability for some assays.
Why should I read this?
Short version: this paper shows personalised mRNA vaccines can fire up long-lived, functional T cells in triple-negative breast cancer — and those T cells can stick around for years. If you work in oncology, immunotherapy or vaccine tech, it’s proper proof that neoantigen RNA–LPX can be safe, manufacturable and immunologically potent in an adjuvant TNBC setting. We read the long methods and data so you don’t have to — but skim the figures and the P1 case if you want the coolest bits on persistence and TCR tracking.
Author style
Punchy: this isn’t incremental — it’s a solid demonstration that individualised mRNA neoantigen vaccines produce broad, high-magnitude and durable T cell immunity in a difficult tumour type. The long-lived, stem-like and cytotoxic T cell populations they characterise make the findings particularly noteworthy and worth digging into for anyone planning combination strategies or adjuvant immunotherapy trials.
Context and relevance
TNBC has a high early recurrence risk and limited targeted options. The study places personalised mRNA neoantigen vaccination as a viable adjuvant strategy that elicits robust cellular immunity even in cancers with low-to-moderate mutation loads. The persistence of stem-like and cytotoxic neoantigen-specific T cells suggests potential synergy with checkpoint blockade or cytokine support and informs mechanisms of relapse and immune escape that should guide future combination trials and patient selection.