
Natural maternal immunity protects neonates from Escherichia coli sepsis
Article metadata
Article Date: 11 March 2026
Article URL: https://www.nature.com/articles/s41586-026-10225-z
Article image: Fig.1
{kind=link}
Summary
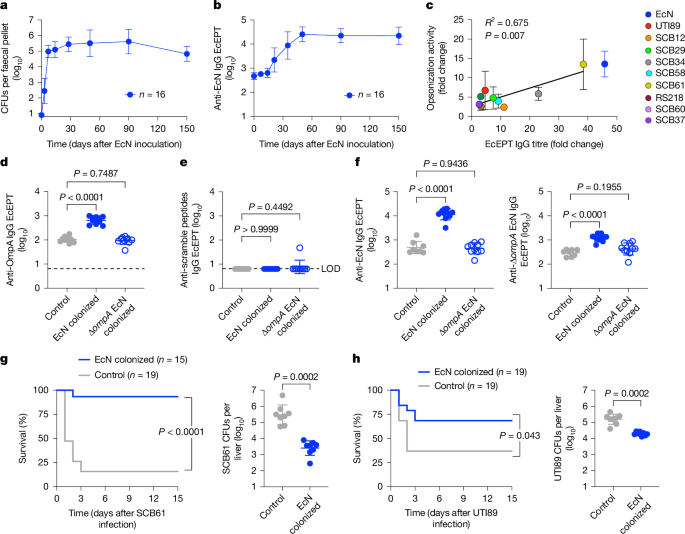
This Nature paper shows that naturally acquired maternal antibodies against Escherichia coli — primed by maternal colonisation with commensal E. coli (notably the probiotic strain Nissle 1917, EcN) — protect newborns from invasive E. coli infection. In mice, EcN colonisation drives systemic IgG (especially IgG1 and IgG2b) that is cross-reactive with clinically relevant E. coli strains and targets conserved outer-membrane proteins such as OmpA. These antibodies are vertically transferred to pups (in utero and via milk) and, by opsonisation that requires complement and Fcγ receptors, sharply reduce bacterial burden and mortality in neonatal infection models.
Importantly, an analysis of human newborn dried blood spots (collected ~24 hours after birth) from 100 babies who later developed neonatal E. coli sepsis showed marked reductions (roughly tenfold) in anti-E. coli IgG titres and reduced IgG-dependent opsonisation compared with matched controls. The work links diminished vertically transferred natural maternal IgG to increased neonatal risk and suggests actionable prevention strategies including prenatal antibody screening, maternal probiotic colonisation or targeted vaccination (OmpA and other outer membrane proteins) and passive immunotherapy.
Key Points
- Maternal colonisation with commensal E. coli Nissle 1917 (EcN) primes systemic anti-E. coli IgG in mice that is cross-reactive with clinical neonatal sepsis isolates.
- OmpA, an outer membrane protein, is a major immunological target of EcN-primed antibodies, but responses are polyclonal and cross-reactive beyond OmpA alone.
- Vertically transferred IgG from EcN-colonised mothers protects neonatal mice from systemic E. coli infection; protection requires antibody, complement (C1q/C3) and Fcγ receptors for opsonisation in neonates.
- Human data from newborn dried blood spots show substantially lower anti-E. coli IgG and opsonisation activity in babies who developed E. coli sepsis versus matched controls, independent of gestational-age effects.
- Risk thresholds for anti-E. coli and anti-OmpA IgG and opsonisation were identified that correlate with increased sepsis risk, suggesting biomarkers for prenatal screening.
- Potential interventions proposed: prenatal screening for anti-E. coli IgG, maternal EcN colonisation or OmpA-targeted vaccines, and targeted passive immunoglobulin therapies for high-risk infants.
Content summary
The authors combined mechanistic mouse studies with human retrospective data. In mice, a single oral EcN inoculation establishes durable intestinal colonisation and raises systemic anti-EcN IgG over weeks. These antibodies opsonise diverse clinical E. coli isolates and reduce mortality and bacterial loads after systemic challenge. Knock-out and transfer experiments demonstrate antibodies are necessary and sufficient for protection; neonatal protection depends on complement and FcγR-mediated opsonisation. Cross-fostering experiments show both prenatal and postnatal transfer contribute, with breastmilk playing an important role in mice.
In humans, the team analysed archived newborn screening dried blood spots from 100 infants with E. coli neonatal sepsis and matched controls. A consistent, large reduction in anti-E. coli IgG (especially IgG2) and reduced IgG-dependent opsonisation were found in cases. These differences were not explained by overall IgG recovery or premature birth alone. The findings point to deficient vertically transferred specific antibodies as a universal risk factor for neonatal E. coli sepsis.
Context and relevance
Neonatal E. coli sepsis remains a leading cause of early-life bacterial mortality, particularly in preterm infants. This study reframes much of neonatal susceptibility as a deficit of specific, vertically transferred natural maternal antibodies rather than only neonatal immune immaturity or pathogen exposure. The translational implications are immediate: prenatal serological screening, focused maternal interventions (probiotics, vaccination) and early passive immunotherapy could reduce incidence. The work is relevant to neonatologists, obstetricians, infectious disease specialists and public-health planners considering prevention strategies for early-onset sepsis.
Author style
Punchy. The paper is a clear, action-oriented mix of rigorous mouse mechanistic data and human newborn specimen analysis. If you work with neonatal infection, maternal–fetal medicine or vaccine strategy, the details are worth reading: they map a plausible route from bench to simple clinical interventions (screening, maternal colonisation or targeted immunotherapy).
Why should I read this?
Quick, no-nonsense take: this explains why some babies — even when exposed to E. coli — go on to get septic. It shows maternal natural IgG (often primed by harmless gut E. coli) is a frontline defence for neonates. That means you can think about screening mums, tweaking maternal microbiota, or using antibody therapies to protect newborns. If you care about reducing early-life sepsis, this paper saves you time — it points to real, testable prevention strategies now.